
Do ACE inhibitors work on afferent or efferent?
By Matthew Harrington
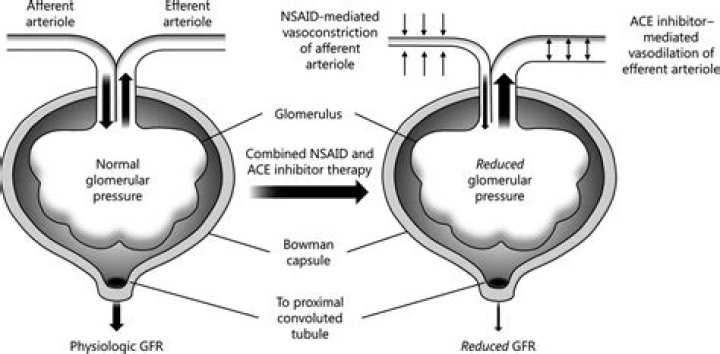
Unlike the direct-acting smooth muscle vasodilators or adrenergic inhibitors, ACE inhibitors dilate the efferent as well as the afferent glomerular arterioles and thereby reduce glomerular hydrostatic pressure and renal filtration fraction, even though renal blood flow and glomerular filtration rate are preserved.
.
Also to know is, why ACE inhibitors are contraindicated in renal failure?
Angiotensin-converting enzyme inhibitors (ACEIs) are contraindicated in patients with bilateral renal artery stenosis due to risk of azotemia resulting from preferential efferent arteriolar vasodilation in the renal glomerulus due to inhibition of angiotensin II.
Secondly, how do ACE inhibitors protect the kidneys? ACE inhibitors and ARBs have been shown effective in preventing or at least slowing the process of renal disease in patients with diabetes by interfering with the renin-angiotensin system. ACE inhibitors and ARBs lower intraglomerular pressure by decreasing efferent arteriolar pressure.
Correspondingly, do ACE inhibitors increase or decrease GFR?
In general, ACE-inhibition does not affect normal glomerular filtration rate (GFR) but may increase GFR in patients on a low sodium intake prior to treatment. Since the rise in GFR is smaller than the rise in renal blood flow, in most instances a decrease in filtration fraction will result.
Do ACE inhibitors damage kidneys?
In conditions in which glomerular filtration is critically dependent on angiotensin II-mediated efferent vascular tone (such as a post-stenotic kidney, or patients with heart failure and severe depletion of circulating volume), ACE inhibition can induce acute renal failure, which is reversible after withdrawal of the
Related Question AnswersWho should not take ACE inhibitors?
The following are people who shouldn't take ACE inhibitors: Pregnant women. An ACE inhibitor might hurt the baby during the last six months of pregnancy. If you were already taking an ACE inhibitor and stop taking it during the first three months of pregnancy, the risk to your baby is very low.Why does creatinine increase with ACE inhibitors?
Chien, DO, Rowland Heights, Calif. Starting an ACE inhibitor can result in small and nonprogressive serum creatinine increases that reflect decreased glomerular filtration rate and reduced intraglomerular pressure.At what GFR do you stop ACE inhibitors?
While these medications are the main pharmacologic therapy for reducing albuminuria in CKD patients, they increase serum creatinine by 20% to 30% and thereby decrease GFR. The decision to continue or discontinue ACEi/ARB use when patients reach CKD stage 4 or 5 is controversial.At what creatinine level should ACE inhibitors be stopped?
The authors recommend that ACE inhibitor therapy should not be discontinued unless serum creatinine level rise above 30% over baseline during the first 2 months after initiation of therapy or hyperkalemia (serum potassium level >or=5.6 mmol/L) develops.Are ACE inhibitors nephrotoxic?
ACE inhibitors are not nephrotoxic. Baseline serum creatinine levels of up to 3.0 mg per dL (27 μmol per L) are generally considered safe.Why do ACE inhibitors decrease GFR?
Increased efferent pressure (due to efferent vasoconstriction) impedes blood flow out of the glomerulus, so GFR is maintained. In addition, ACE inhibitors slow the progression of diabetic nephropathy & reduce proteinuria INDEPENDENT of their effect on blood pressure.How effective are ACE inhibitors?
Overall, ACE inhibitors had a modest collective effect in reducing blood pressure. The mean reduction in systolic blood pressure ranged between 6 mm Hg and 9 mm Hg, and the mean reduction in diastolic blood pressure was 4-5 mm Hg.Can ACE inhibitors increase creatinine levels?
The rise in serum creatinine values usually begins a few days after beginning therapy with an ACE inhibitor or an ARB, as angiotensin II levels are rapidly reduced or blocked from binding. A larger rise in creatinine level is likely to occur in patients with bilateral renovascular disease, CKD, and heart failure.How do ACE inhibitors cause nephrotoxicity?
ACE inhibitors depress A-II and thus inhibit A-II-mediated vasoconstriction. This lowers glomerular filtration pressure and decreases the glomerular filtration rate. NSAIDs and ACE inhibitors are the main causes of drug-induced ARF in the elderly5.What are the side effects of ACE inhibitors?
What Are the Side Effects of ACE Inhibitors?- Cough .
- Red, itchy skin or rash.
- Dizziness , lightheadedness or faintness upon rising.
- Salty or metallic taste or a decreased ability to taste.
- Physical symptoms.
- Swelling of your neck, face, and tongue.
- High potassium levels.
- Kidney failure.



